

Last updated: 4/19/2021
Application For Mediation Or Hearing-Form A {WC-104A}
Start Your Free Trial $ 13.99What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
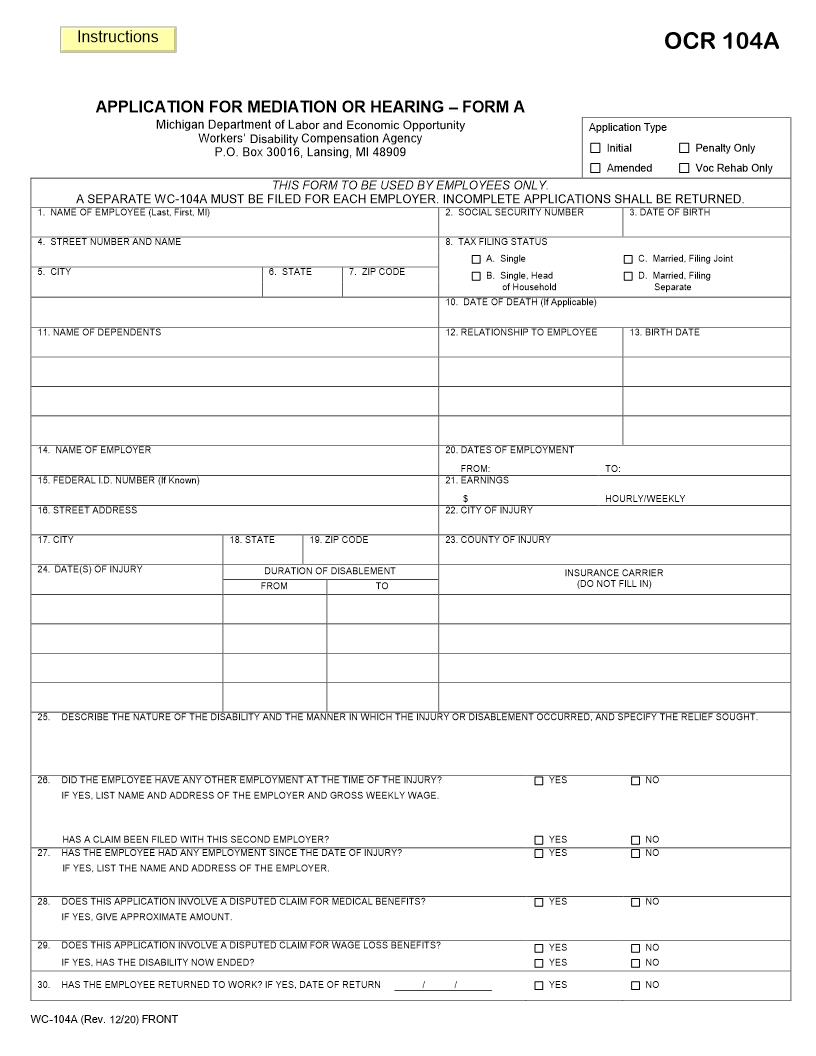
APPLICATION FOR MEDIATION OR HEARING FORM A Michigan Department of Licensing and Regulatory Affairs Workers' Compensation Agency P.O. Box 30016, Lansing, MI 48909 Application Type Initial Amended Penalty Only Voc Rehab Only 1. NAME OF EMPLOYEE (Last, First, MI) 4. STREET NUMBER AND NAME 5. CITY 9. SEX Male Female 11. NAME OF DEPENDENTS THIS FORM TO BE USED BY EMPLOYEES ONLY. A SEPARATE WC-104A MUST BE FILED FOR EACH EMPLOYER. INCOMPLETE APPLICATIONS SHALL BE RETURNED. 2. SOCIAL SECURITY NUMBER 8. TAX FILING STATUS A. Single 6. STATE 7. ZIP CODE B. Single, Head of Household 10. DATE OF DEATH (If Applicable) 12. RELATIONSHIP TO EMPLOYEE 13. BIRTH DATE C. Married, Filing Joint D. Married, Filing Separate 3. DATE OF BIRTH 14. NAME OF EMPLOYER 15. FEDERAL I.D. NUMBER (If Known) 16. STREET ADDRESS 17. CITY 24. DATE(S) OF INJURY 18. STATE 19. ZIP CODE 20. DATES OF EMPLOYMENT FROM: 21. EARNINGS $ 22. CITY OF INJURY 23. COUNTY OF INJURY INSURANCE CARRIER (DO NOT FILL IN) TO: HOURLY/WEEKLY DURATION OF DISABLEMENT FROM TO 25. DESCRIBE THE NATURE OF THE DISABILITY AND THE MANNER IN WHICH THE INJURY OR DISABLEMENT OCCURRED, AND SPECIFY THE RELIEF SOUGHT. 26. DID THE EMPLOYEE HAVE ANY OTHER EMPLOYMENT AT THE TIME OF THE INJURY? IF YES, LIST NAME AND ADDRESS OF THE EMPLOYER AND GROSS WEEKLY WAGE. YES NO 27. HAS A CLAIM BEEN FILED WITH THIS SECOND EMPLOYER? HAS THE EMPLOYEE HAD ANY EMPLOYMENT SINCE THE DATE OF INJURY? IF YES, LIST THE NAME AND ADDRESS OF THE EMPLOYER. YES YES NO NO 28. DOES THIS APPLICATION INVOLVE A DISPUTED CLAIM FOR MEDICAL BENEFITS? IF YES, GIVE APPROXIMATE AMOUNT. YES NO 29. DOES THIS APPLICATION INVOLVE A DISPUTED CLAIM FOR WAGE LOSS BENEFITS? IF YES, HAS THE DISABILITY NOW ENDED? YES YES NO NO NO 30. HAS THE EMPLOYEE RETURNED TO WORK? IF YES, DATE OF RETURN / / YES WC-104A (Rev. 2/13) FRONT American LegalNet, Inc. www.FormsWorkFlow.com 31. 32. 33. IS THIS A CASE IN WHICH WAGE LOSS BENEFITS WERE PAID VOLUNTARILY AND HAVE BEEN TERMINATED WITHIN THE LAST 60 DAYS? DOES THIS INVOLVE A CLAIM FOR VOCATIONAL REHABILITATION SERVICES? IS A CLAIM BEING MADE AGAINST ONE OF THE FUNDS? IF YES, PLEASE SPECIFY THE NAME OF THE FUND AND THE SPECIFIC PROVISION OF THE ACT. YES YES YES NO NO NO 34. OTHER BENEFITS (Please indicate which of the following benefits you are or have received based on employment with this employer during the periods of disability indicated on this application) A. B. C. D. 35. OLD AGE SOCIAL SECURITY ____________________ WEEKLY/MONTHLY PENSION OR RETIREMENT PLAN ________________ WEEKLY/MONTHLY SICK AND ACCIDENT INSURANCE _______________ WEEKLY/MONTHLY WAGE CONTINUATION PLAN ___________________ WEEKLY/MONTHLY E. F. G. H. UNEMPLOYMENT BENEFITS __________________ WEEKLY/MONTHLY DISABILITY INSURANCE POLICY _______________ WEEKLY/MONTHLY SELF INSURANCE PLAN ______________________ WEEKLY/MONTHLY PROFIT SHARING PLAN ______________________ WEEKLY/MONTHLY LIST THE NAMES AND ADDRESSES OF DOCTORS, HOSPITALS AND OTHER HEALTH CARE PROVIDERS WHO TREATED YOU FOR ANY DATE(S) OF INJURY LISTED IN #24. NAME ADDRESS (Street Number and Name) CITY STATE ZIP CODE 36. LIST THE NAMES AND ADDRESSES OF ANY WITNESSES. (Do not list names of witnesses who are currently employed by the named employer) NAME ADDRESS (Street Number and Name) CITY STATE ZIP CODE 37. I INTEND TO CALL WITNESSES WHO ARE CURRENTLY EMPLOYED BY THE NAMED EMPLOYER. Yes No Making a false or fraudulent statement for the purpose of obtaining or denying benefits can result in criminal or civil prosecution, or both, and denial of benefits. CERTIFICATION AND SIGNATURE AUTHORITY: Workers' Disability Compensation Act, 418.222; 418.847; R 408.34 COMPLETION: Voluntary PENALTY: None I HEREBY CERTIFY THAT THE ABOVE INFORMATION IS TRUE TO THE BEST OF MY KNOWLEDGE. I ALSO CERTIFY THAT I HAVE, AS OF THIS DATE, MAILED TO MY EMPLOYER OR ITS INSURANCE CARRIER COPIES OF ANY MEDICAL RECORDS RELEVANT TO THIS CLAIM THAT ARE IN MY POSSESSION. SIGNATURE OF APPLICANT TELEPHONE NUMBER ( ) DATE NAME OF ATTORNEY ATTORNEY IDENTIFICATION NAME OF LAW FIRM CITY TELEPHONE NUMBER ( ) ATTORNEY I.D. P ADDRESS (Street Number and Name) SIGNATURE OF ATTORNEY STATE DATE ZIP CODE WC-104A (Rev. 2/13) BACK American LegalNet, Inc. www.FormsWorkFlow.com
Related forms
-

Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/5 Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/ -
Michigan/Workers Comp/