

Last updated: 11/15/2007
Unreimbursed Medical Expense Form
Start Your Free Trial $ 13.99What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
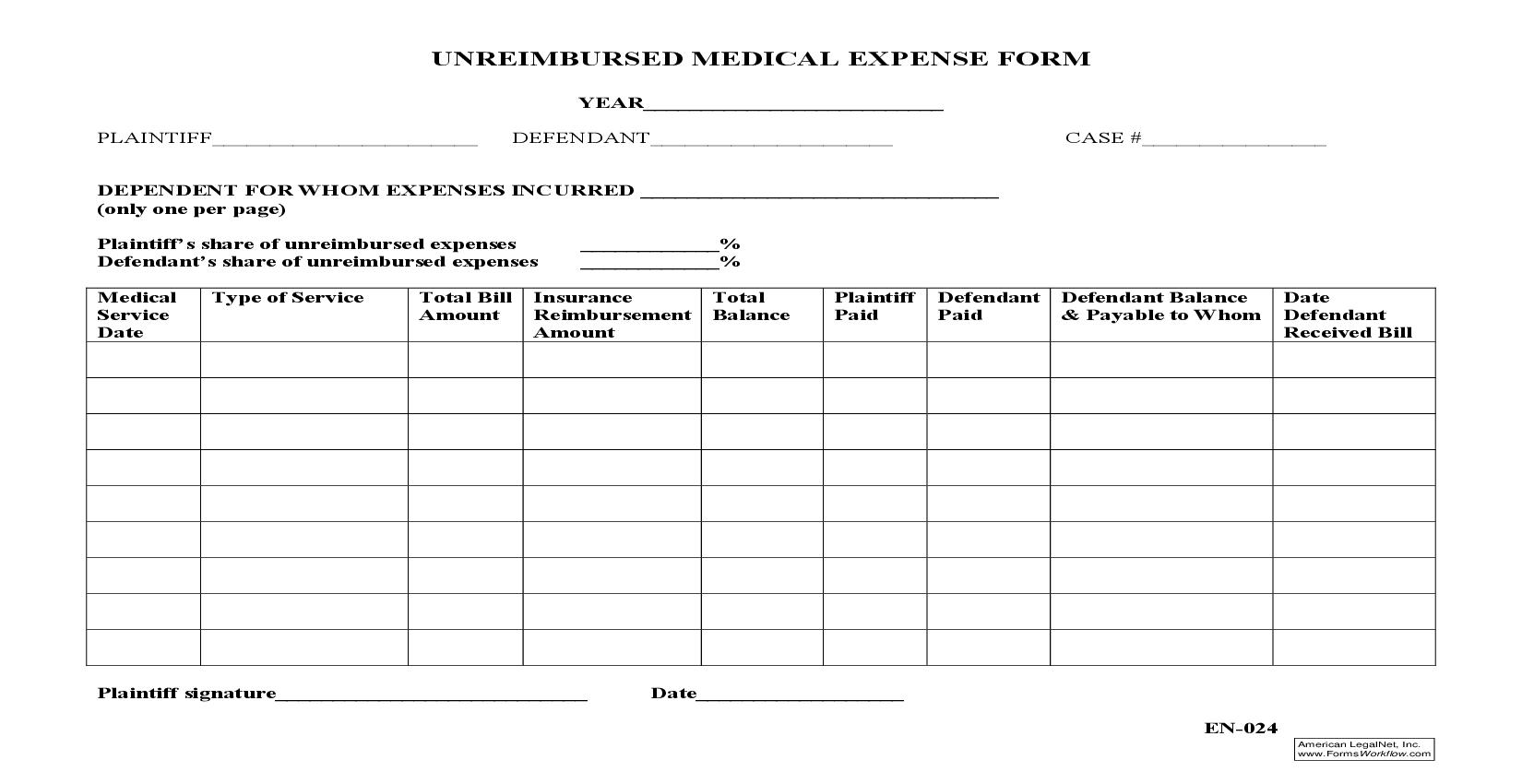
UNREIMBURSED MEDICAL EXPENSE FORM YEAR__________________________ PLAINTIFF_______________________ DEFENDANT_____________________ CASE #________________ DEPENDENT FOR WHOM EXPENSES INCURRED _______________________________ (only one per page) Plaintiff's share of unreimbursed expenses Defendant's share of unreimbursed expenses Medical Service Date Type of Service ____________% ____________% Plaintiff Defendant Defendant Balance Date Paid Paid & Payable to Whom Defendant Received Bill Total Bill Insurance Total Amount Reimbursement Balance Amount Plaintiff signature___________________________ Date__________________ EN-024 American LegalNet, Inc. www.FormsWorkflow.com
Related forms
-

Pennsylvania/Local County/Berks/Domestic Relations/ -
Pennsylvania/Local County/Berks/Domestic Relations/ -
Pennsylvania/Local County/Berks/Domestic Relations/ -
Pennsylvania/Local County/Berks/Domestic Relations/ -
Pennsylvania/Local County/Berks/Domestic Relations/ -
Pennsylvania/Local County/Berks/Domestic Relations/