

Last updated: 1/13/2020
Work Status Report {DWC-73}
Start Your Free Trial $ 13.99What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
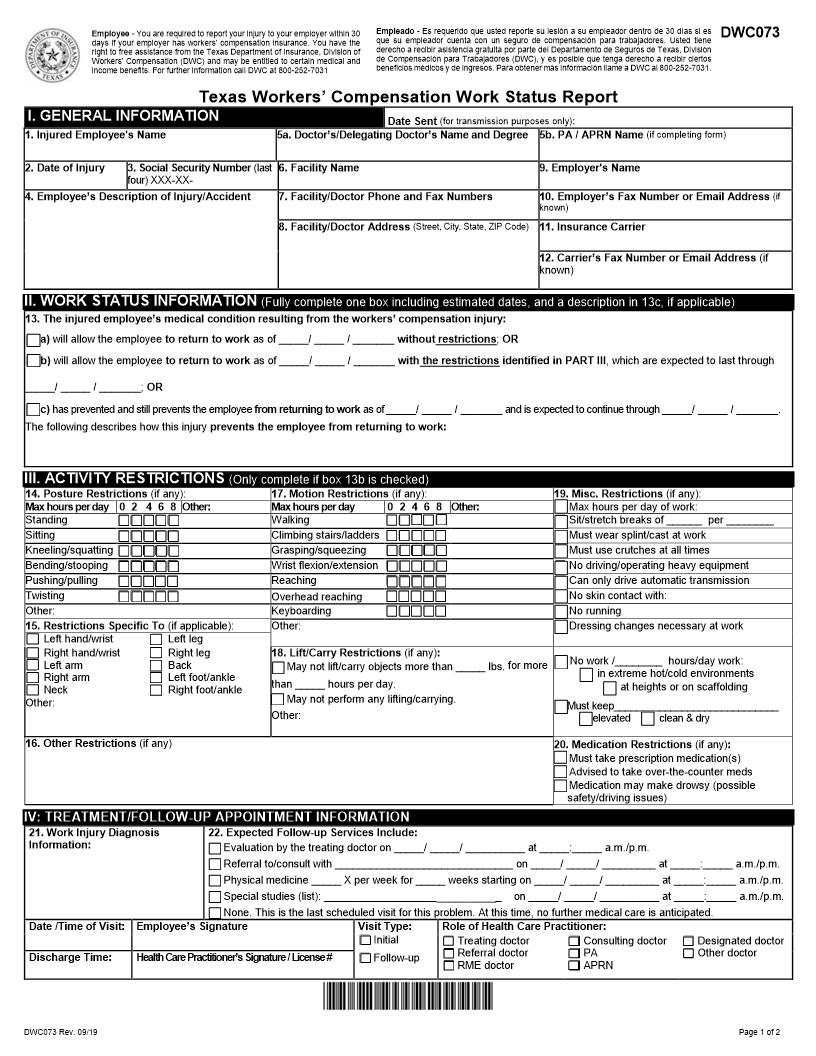
DWC073 DWC073 Rev. 10/18 Page 1 of 2 Texas Workers222 Compensation Work Status Report I. GENERAL INFORMATION Date Sent (for transmission purposes only) : 1. Injured Employee's Name 5 a . Doctor222s Name and Degree or Delegating Doctor and Degree 5b . Physician Assistant Name (if completing for m) 2.Date of Injury 3. Social Security Number (last four ) XXX-XX- 6 .Facility Name 9 .Employer's Name 4.Employee222s Description of Injury/Accident 7 .Facility/Doctor Phone and Fax Numbers 1 0 .Employer222s Fax Number or Email Address (if k nown) 8 .Fa cility/Doctor Address (Street, City, State, ZIP Code) 1 1 . Insurance Carrier 1 2 .Carrier222s Fax Number or Email Address (if known) II.WORK STATUS INFORMATION (Fully complete one box including estimated dates, and a description in 13c, if applicable) 1 3 .The injured employee222s medical condition resulting from the workers222 compensation injury: a)will allow the employee to return to work as of / / without restrictions; OR b)will allow the employee to return to work as of / / with the restrictions identified in PART III, which are expected to last through / / ; OR c) has prevented and still prevents the employee from returning to work as of / / and is expected to continue through / / . The following describes how this injury prevents the employee from returning to work: III.ACTIVITY RESTRICTIONS (Only complete if box 13b is checked) 14.Posture Restrictions (if any): 17.Motion Restrictions (if any): 19.Misc. Restrictions (if any): Max h ours per da y 0 2 4 6 8 Other: Max h ours per day 0 2 4 6 8 Other: Max hours per day of work: Standing Walking Sit/ s tretch breaks of per Si tting Climbing stairs/ladders Must wear splint/cast a t work Kneeling/ s quatting Grasping/ s queezing Must us e crutches at all times Bending/ s tooping Wrist flexion/extension No driving/operating heavy equipment Pushing/ p ulling Reaching Can only drive automatic transmission Twisting Overhead r eaching No skin contact with: Other: Keyboarding No running 15.Restrictions Specific To (if applicab le): Other: Dressing changes necessary at work Left h and/ w rist Right hand/wrist Left arm Right arm Neck Left l eg Right leg Back Left foot/ankle Right f oot/ a nkle 18.Lift/Carry Restrictions (if any) : May not lift/carry objects more than lbs. for more than hours per day . May not perform any lifting/carrying. Other: No work / hours/day work: in extreme hot/cold environments at heights or on scaffolding Must keep elevated clean & dry Other: 1 6 .O ther R estrictions (if any) 20.Medication Restrictions (if any) : Must take prescription medication(s) Advised to take over-the-counter meds Medication may make drowsy (possible safety/driving issues) IV: TREATMENT/FOLLOW-UP APPOINTMENT INFORMATION 21.Work Injury Diagnos is Information: 22. Expected Follow-up Services Include:Evaluation by the treating doctor on / / at : a.m./p.m.Referral to/consult with on / / at : a.m./p.m.Physical medicine X per week for weeks starting on / / at : a.m./p.m.Special studies (list): on / / at : a.m./p.m.None. This is the last scheduled visit for this problem. At this time, no further medical care is anticipated. Date /Time of Visit: Employee222s Signature Visit Type: Initial Follow-up Role of Health Care Practitioner: Treating doctor Referral doctor RME doctor Consulting doctor Physician assistant Designated doctor Other doctor Discharge Time: Health Care Practitioner222s Signature / License # Employee - You are required to report your injury to your emplo yer within 30 days if your employer has workers222 compensation insurance. You have the right to free assistance from the Texas Department of Insurance, Division of Workers222 Compensation (DWC) and may be entitled to certain medical and income benefits. For f urther information call DWC at 800 - 252 - 7031 Empleado - Es requerido que usted reporte su lesi363n a su empleador dentro de 30 d355as si es que su empleador cuenta con un seguro de com pensaci363n para trabajadores. Usted tiene derecho a recibir asistencia gratuita por parte del Departamento de Seguros de Texas, Divisi363n de Compensaci363n para Trabajadores (DWC), y es posible que tenga derecho a recibir ciertos beneficios m351dicos y de ingres os. Para obtener m341s informaci363n llame a DWC al 800 - 252 - 7031. American LegalNet, Inc. www.FormsWorkFlow.com DWC073 DWC073 Rev. 10/18 Page 2 of 2Frequently Asked Questions Work Status Report (DWC Form-073) Under what circumstances am I required to file DWC Form-073? Filing requirements for DWC Form-073 vary depending on the type of doctor filing the Work Status Report. The specific requirements are shown in the chart below. Type of Doctor When to File DWC Form-073 Where to File Delivery Method Deadline Treating Doctor Referral Doctor Or Delegated Physician Assistant after the initial examination of the injured employee, regardless of the employee222s work status when there is a change in the injured employee222swork statuswhen there is a substantial change in the injuredemployee222s activity restrictionson a schedule requested by the insurance carrieras long as it is based on the injured employee222sscheduled appointments with the doctor (not toexceed one report every two weeks) injured employee hand deliver ; electronic transmission, with agreement (fax, email, or similar method) at the time of the examination insurance carrier electronic transmission within 2 working days of the examination employer electronic t ransmission unless recipient has not provided a fax number or email address; then by personal delivery or mail after receiving a set of functional job descriptions from the employer or insurance carrier listingmodified duty positions, including the physicaland time requirements of the positions, that theemployer has available for the injured employeeto work after receiving a DWC Form-073 from a requiredmedical exam (RME) doctor that indicates theinjured employee can return to work with orwithout restrictions injured employee hand deliver unless no appointment is scheduled before deadline; then electronic transmission unless recipient has not provided a fax number or email address; then by mail within 7 days of receiving job description or RME opinion insurance carrier employer electronic transmission Designated Doctor after examination of an injured employee to address any question relating to return to work NOTE: The designated doctor must file a narrative report along with DWC Form-073. injured employee injured employee222srepresentative (if any) electronic transmission unless recipient has not provided a fax number or email address; then by other verifiable means within 7 working days of the examination insurance carrier treating doctor electronic transmission division fax to 512 - 490 - 1047 RME Doctor after examination of an injured employee (subsequent to a Designated Doctor'sexamination), if the RME doctor determines that theinjured employee can return to work immediatelywith or without restrictions injured employee injured employee222srepresentative (if any) electronic transmission unless recipient has not provided a fax number or email address; then by other verifiable means within 7 days of the examination insu rance carrier treating doctor electronic transmission Where can I find more information about DWC Form-073? For complete requirements regarding the filing of this report, see 28 Texas Administrative Code 247247126.6, 127.10, and 129.5. These rules are available on the TDI website at http://www.tdi.texas.gov/wc/rules/index.html . If you have additional questions, call Comp Connection for Health Care Providers at 1-800-372-7713 (512-804-4000 in the Austin area) and select option 3. NOTE: With few exceptions, upon your request, you are entitled to be informed about the information DWC collects about you; to get and review the information (Government Code 247247552.021 and 552.023); and to have DWC correct information that is incorrect (Government Code, 247559.004). For more information, contact agencycounsel@tdi.texas.gov or you may refer to the Corrections Procedure section at www.tdi.texas.gov . American LegalNet, Inc. www.FormsWorkFlow.com
Related forms
-

Texas/Workers Compensation/Medical/ -
Texas/Workers Compensation/Medical/ -
Texas/6 Workers Compensation/Medical/ -
Texas/Workers Compensation/Medical/ -
Texas/Workers Compensation/Medical/ -
Texas/Workers Compensation/Medical/ -
Texas/Workers Compensation/Medical/ -
Texas/Workers Compensation/Medical/ -
Texas/Workers Compensation/Medical/ -
Texas/Workers Compensation/Medical/