

Last updated: 6/3/2022
Description Of Injured Employees Employment {DWC-74}
Start Your Free Trial $ 13.99What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
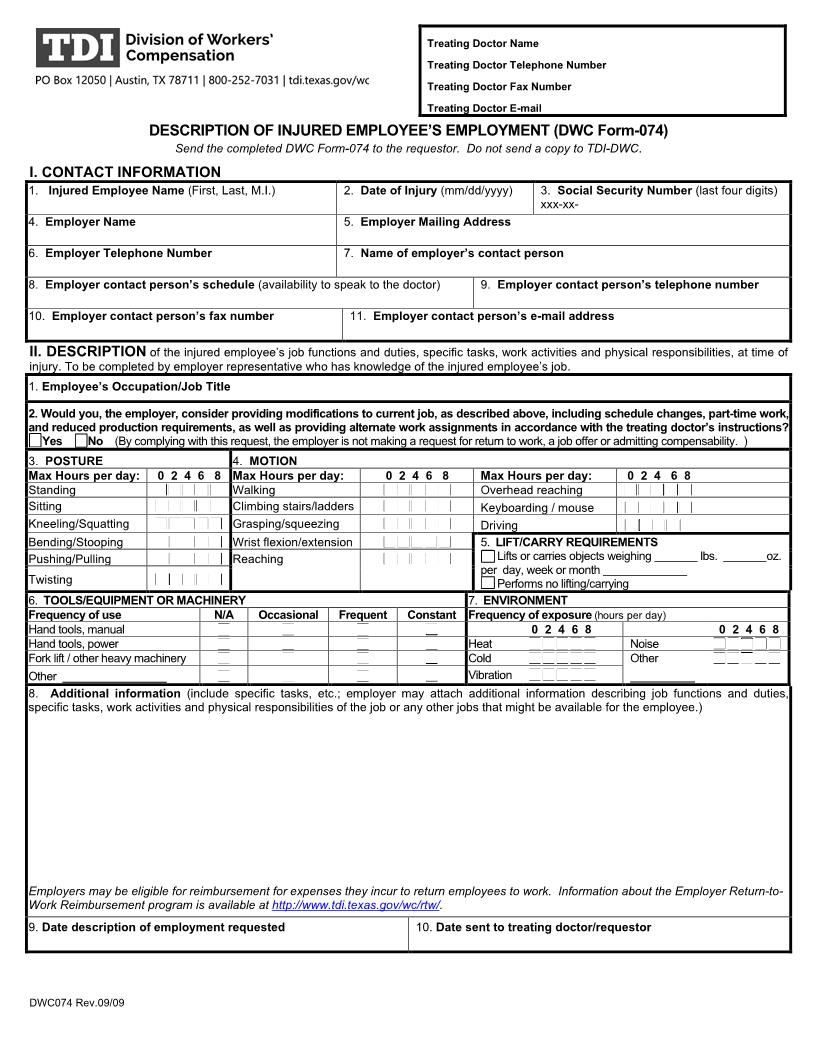
Texas Department Of Insurance Division of Workers' Compensation 7551 Metro Center Dr., Ste.100 Austin, TX 78744-1609 (512) 804-4000 (512) 804-4378 fax www.tdi.texas.gov Treating Doctor Name Treating Doctor Telephone Number Treating Doctor Fax Number Treating Doctor E-mail DESCRIPTION OF INJURED EMPLOYEE'S EMPLOYMENT (DWC Form-074) Send the completed DWC Form-074 to the requestor. Do not send a copy to TDI-DWC. I. CONTACT INFORMATION 1. Injured Employee Name (First, Last, M.I.) 4. Employer Name 6. Employer Telephone Number 2. Date of Injury (mm/dd/yyyy) 5. Employer Mailing Address 7. Name of employer's contact person 9. Employer contact person's telephone number 3. Social Security Number (last four digits) xxx-xx- 8. Employer contact person's schedule (availability to speak to the doctor) 10. Employer contact person's fax number 11. Employer contact person's e-mail address II. DESCRIPTION of the injured employee's job functions and duties, specific tasks, work activities and physical responsibilities, at time of injury. To be completed by employer representative who has knowledge of the injured employee's job. 1. Employee's Occupation/Job Title 2. Would you, the employer, consider providing modifications to current job, as described above, including schedule changes, part-time work, and reduced production requirements, as well as providing alternate work assignments in accordance with the treating doctor's instructions? Yes No (By complying with this request, the employer is not making a request for return to work, a job offer or admitting compensability. ) 3. POSTURE Max Hours per day: Standing Sitting Kneeling/Squatting Bending/Stooping Pushing/Pulling Twisting 4. MOTION 0 2 4 6 8 Max Hours per day: Walking Climbing stairs/ladders Grasping/squeezing Wrist flexion/extension Reaching 0246 8 Max Hours per day: 024 68 Overhead reaching Keyboarding / mouse Driving 5. LIFT/CARRY REQUIREMENTS Lifts or carries objects weighing lbs. x per day, week or month Performs no lifting/carrying 7. ENVIRONMENT Constant Frequency of exposure (hours per day) 02468 02468 Heat Noise Other Cold Vibration 6. TOOLS/EQUIPMENT OR MACHINERY Frequency of use N/A Occasional Frequent Hand tools, manual Hand tools, power Fork lift / other heavy machinery Other 8. Additional information (include specific tasks, etc.; employer may attach additional information describing job functions and duties, specific tasks, work activities and physical responsibilities of the job or any other jobs that might be available for the employee.) Employers may be eligible for reimbursement for expenses they incur to return employees to work. Information about the Employer Return-toWork Reimbursement program is available at http://www.tdi.texas.gov/wc/rtw/. 9. Date description of employment requested 10. Date sent to treating doctor/requestor DWC074 Rev.09/09 American LegalNet, Inc. www.FormsWorkFlow.com Instructions for Completing DESCRIPTION OF INJURED EMPLOYEE EMPLOYMENT (DWC Form-074) What is the purpose of the DWC Form-074, Description of Injured Employee Employment? The purpose of the form is to facilitate the exchange of information between the employer and injured employee's treating doctor regarding the job functions and duties, specific tasks, work activities and physical responsibilities of an injured employee's job at the time of injury and return the injured employee to employment as soon as it is considered safe and appropriate by the treating doctor. Who should complete the DWC-074? The form should be completed by an employer representative who has actual knowledge of the injured employee's job requirements, job functions and physical responsibilities. Where does the employer send the completed form? The employer should send the completed DWC Form-074 to the treating doctor or originating requestor. The employer should retain a copy of the completed form for their records. Do not send a copy of the completed DWC-Form 074 to the Texas Department of Insurance, Division of Workers' Compensation (TDI-DWC). Does completing the DWC Form-074 constitute a request to return to work, a job offer, or an admission of compensability? No, by completing and returning the DWC- Form 074 to the treating doctor or originating requestor, the employer is not making a request to return to work, a job offer, or admitting compensability. Can the employer provide additional information along with the DWC Form-074 in responding to a request for description of an injured employee's employment? Yes, when completing the DWC Form-074, the employer is encouraged to provide additional information that they would like the treating doctor to consider in Box 8, including information about the job the employee had at the time of the injury, and also any other jobs that the employer may have to offer. The employer may attach a job description identifying job functions and physical responsibilities or any other related documentation to the form. NOTE: With few exceptions, you are entitled on request to be informed about the information that TDIDWC collects about you. Under Texas Government Code §552.021 and §552.023 of the Texas Government Code, you are entitled to receive and review the information. Under §559.004 of the Texas Government Code you are entitled to have TDI-DWC correct information about you that is incorrect. For more information, call your local TDI-DWC field office at 800-252-7031. DWC074 Rev. 09/09 Instructions American LegalNet, Inc. www.FormsWorkFlow.com
Related forms
-

Texas/Workers Compensation/Medical/ -
Texas/Workers Compensation/Medical/ -
Texas/6 Workers Compensation/Medical/ -
Texas/Workers Compensation/Medical/ -
Texas/Workers Compensation/Medical/ -
Texas/Workers Compensation/Medical/ -
Texas/Workers Compensation/Medical/ -
Texas/Workers Compensation/Medical/ -
Texas/Workers Compensation/Medical/ -
Texas/Workers Compensation/Medical/