

Last updated: 6/26/2023
Request For Further Action By Legal Counsel {RFA-1LC}
Start Your Free Trial $ 13.99What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
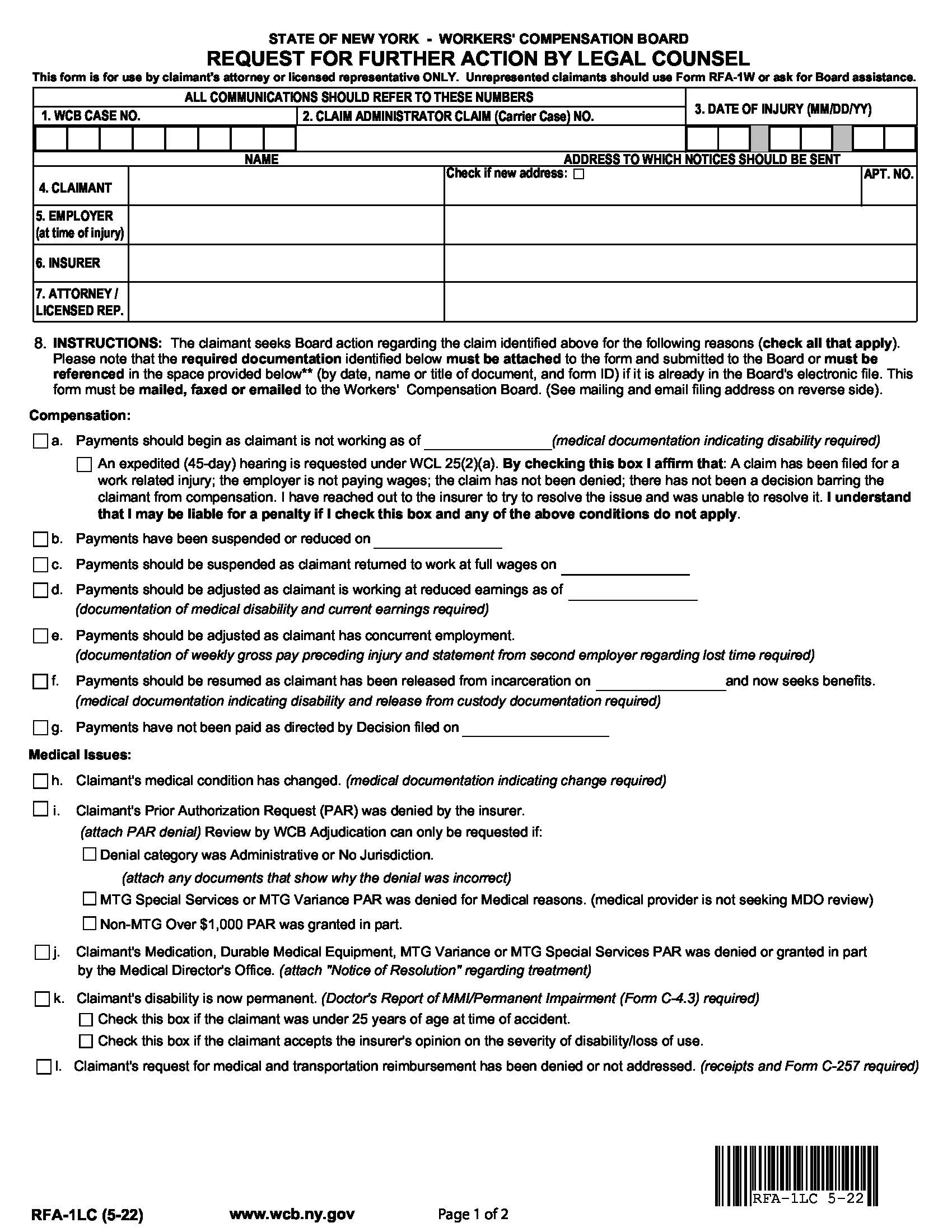
RFA-1LC - REQUEST FOR FURTHER ACTION BY LEGAL COUNSEL. This form is for use by claimant's attorney or licensed representative ONLY. Unrepresented claimants should use Form RFA-1W or ask for Board assistance. You may file this form with the Workers' Compensation Board when you want the Board to take a specific action in your client’s case, or if you need to alert the Board to any problem or situation that is affecting your client’s case. Many of the most frequently requested actions/ situations are contained in Section 8.However, you are not limited to those listed. Check all that apply and/or additional information or explanation in the space provided (p).If an attorney/licensed representative fee is requested, submit Form OC-400.1.Please note: in order to receive an expedited (45-day hearing) you must check box ‘a’ and enter the date the claimant stopped working, AND you must check the box below it for “An expedited (45-day) hearing is requested under WCL 25(2)(a). Complete the identifying information at the top of Form RFA-1LC and send the form, WITH ALL APPLICABLE EVIDENCE ATTACHED, to the Workers' Compensation Board (see address below) The Board will contact you and all parties when it takes action on your client's case. YOU MUST CERTIFY THAT YOU HAVE DISCUSSED THE ISSUE(S) OR ATTEMPTED TO CONTACT THE INSURER/EMPLOYER AND HAVE BEEN UNABLE TO SETTLE THE OUTSTANDING ISSUE(S). YOU MUST SEND A COPY OF THIS FORM TO YOUR CIENT, THE INSURER(S) OR DIRECTLY TO THE EMPLOYER OR TS THIRD PARTY ADMINISTRATOR IF THE EMPLOYER IS SELF-INSURED. www.FormsWorkflow.com
Related forms
-

New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/