

Last updated: 2/6/2024
Notice And Proof Of Claim For Disability Benefits {DB-450}
Start Your Free Trial $ 13.99What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
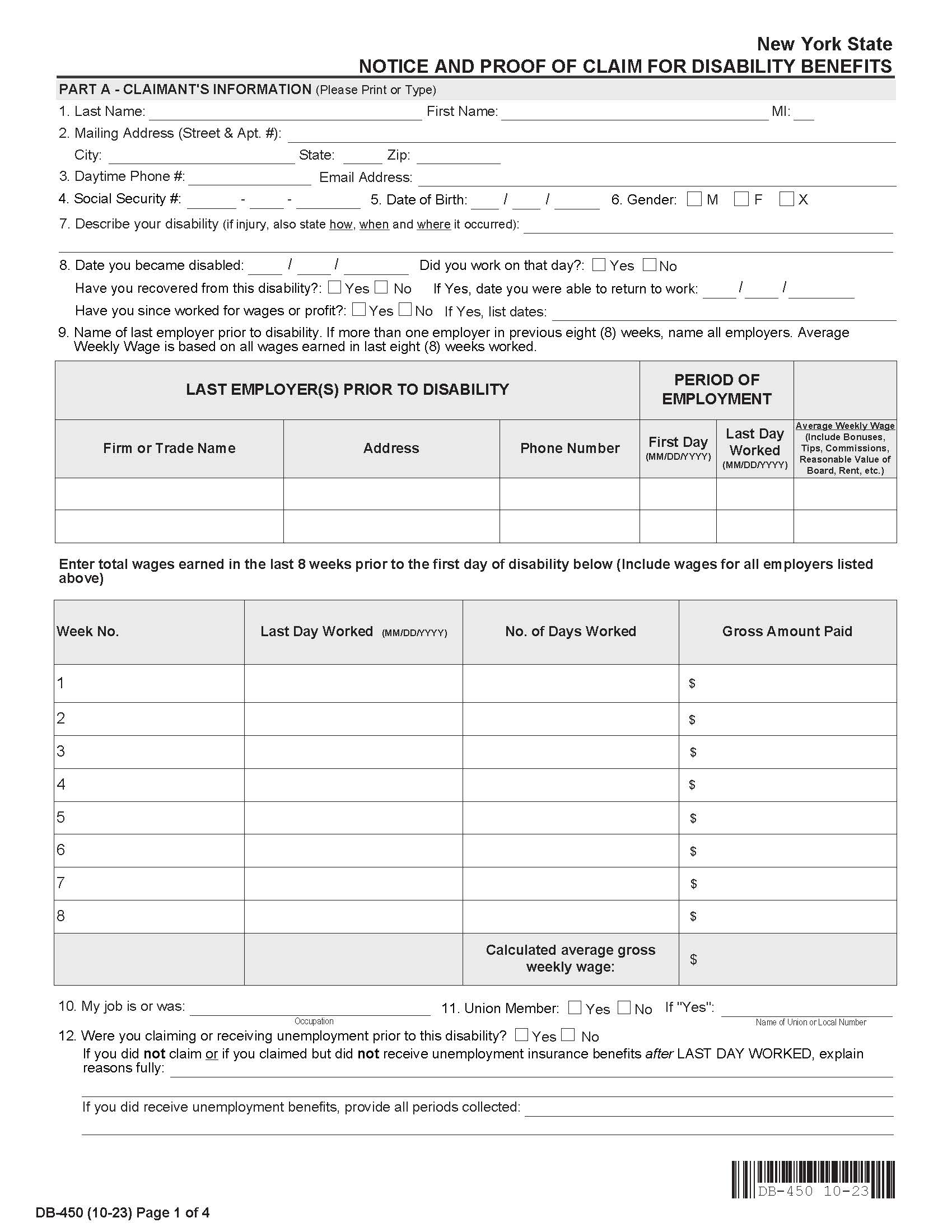
DB-450 - NOTICE AND PROOF OF CLAIM FOR DISABILITY BENEFITS. Do not submit this form prior to your first date of disability. You must submit your completed claim form within 30 calendar days of your first day of disability to avoid losing benefits. Keep a copy of all forms and documentations for your records. 1. If you are using this form because you became disabled while employed or you became disabled within four (4) weeks after termination of employment, your completed claim should be submitted to your employer or your last employer's insurance carrier. 2. If you are using this form because you became disabled after having been unemployed for more than four (4) weeks after termination of employment, your completed claim MUST be mailed to: Workers’ Compensation Board, Disability Benefits Bureau, PO Box 9029, Endicott, NY 13761-9029. If you answered “Yes” to question 13.B.4., please complete and attach Form DB-450.1. Note: This form has a section to be filled out by your healthcare provider, and a section to be completed by your employer. Before providing the form to your employer, fill out your section and make a copy to keep. • The health care provider is required to return the form to you with Part B completed within seven days. If there is a delay, you must wait to submit the form to your insurance carrier. If Part B is not complete (or has incomplete answers) there may be delay in the payment of benefits. • Your employer is required to return the form to you with Part C completed within three business days. If there is a delay, you do not have to wait to proceed – you should send the form to your insurance carrier. They cannot deny your request for disability benefits solely because your employer failed to fill out their section. www.FormsWorkflow.com
Related forms
-

New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/