

Last updated: 5/2/2006
Health Insurers Request For Reimbursement {HIMP-1}
Start Your Free Trial $ 13.99What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
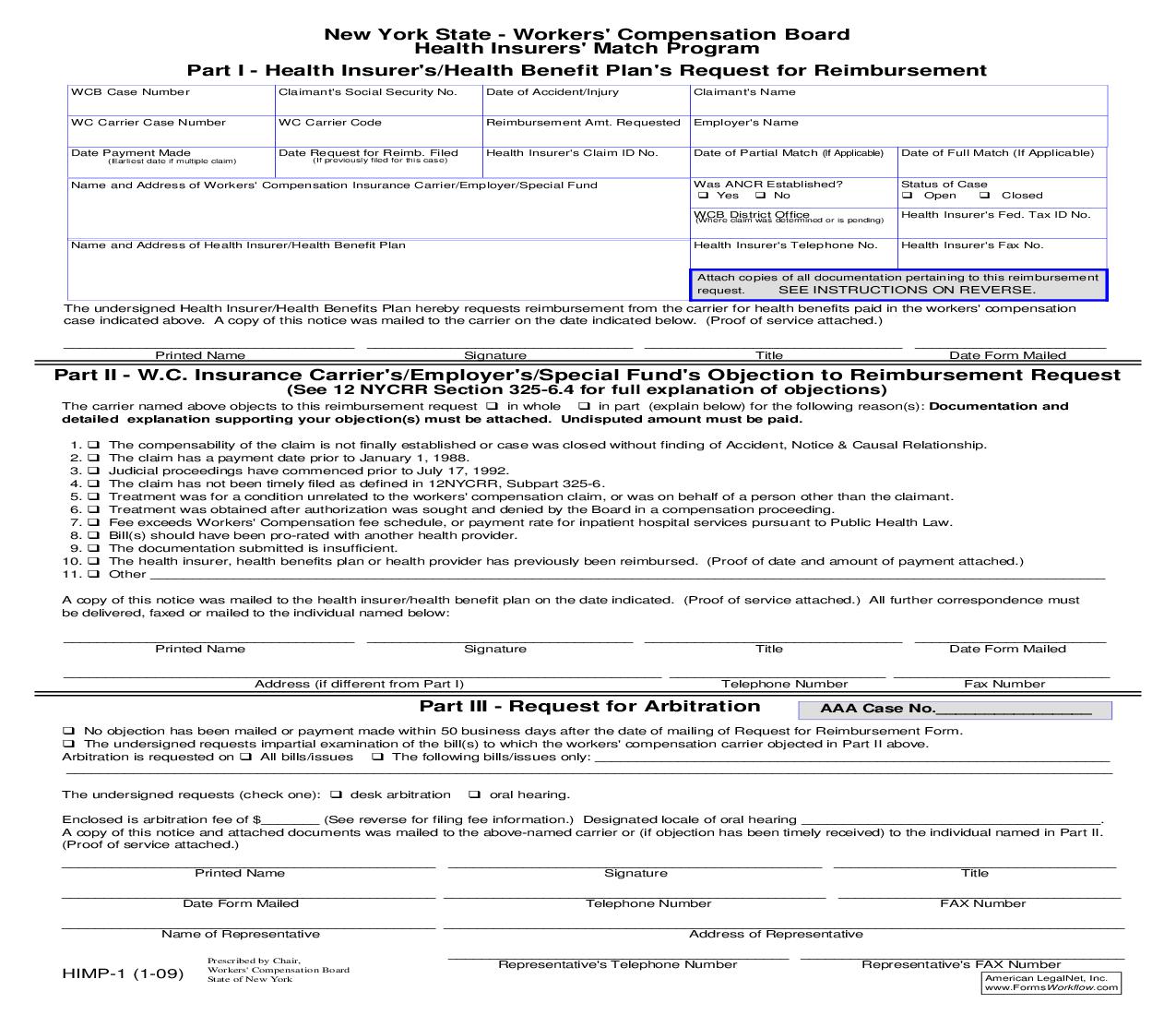
New York State - Workers Compensation Board Health Insurers Match Program Part I - Health Insurers/Health Benefit Plans Request for Reimbursement WCB Case Number Claimants Social Security No.Date of Accident/Injury Claimants Name WC Carrier Case Number WC Carrier Code Reimbursement Amt. Requested Employers Name Date Payment Made Date Request for Reimb. FiledHealth Insurers Claim ID No.Date of Partial Match (If Applicable)Date of Full Match (If Applicable) (Earliest date if multiple claim)(If previously filed for this case) Name and Address of Workers Compensation Insurance Carrier/Employer/Special Fund Was ANCR Established? Status of Case q Yes q No q Open q Closed WCB District Office Health Insurers Fed. Tax ID No. (Where claim was determined or is pending) Name and Address of Health Insurer/Health Benefit Plan Health Insurers Telephone No.Health Insurers Fax No. Attach copies of all documentation pertaining to this reimbursement request. SEE INSTRUCTIONS ON REVERSE. The undersigned Health Insurer/Health Benefits Plan hereby requests reimbursement from the carrier for health benefits paid in the workers compensation case indicated above. A copy of this notice was mailed to the carrier on the date indicated below. (Proof of service attached.) ___________________________________ ________________________________ _______________________________ _______________________ Printed Name Signature Title Date Form MailedPart II - W.C. Insurance Carriers/Employers/Special Funds Objection to Reimbursement Request (See 12 NYCRR Section 325-6.4 for full explanation of objections) The carrier named above objects to this reimbursement request q in whole q in part (explain below) for the following reason(s): Documentation and detailed explanation supporting your objection(s) must be attached. Undisputed amount must be paid. 1. q The compensability of the claim is not finally established or case was closed without finding of Accident, Notice & Causal Relationship. 2. q The claim has a payment date prior to January 1, 1988. 3. q Judicial proceedings have commenced prior to July 17, 1992. 4. q The claim has not been timely filed as defined in 12NYCRR, Subpart 325-6. 5. q Treatment was for a condition unrelated to the workers compensation claim, or was on behalf of a person other than the claimant. 6. q Treatment was obtained after authorization was sought and denied by the Board in a compensation proceeding. 7. q Fee exceeds Workers Compensation fee schedule, or payment rate for inpatient hospital services pursuant to Public Health Law. 8. q Bill(s) should have been pro-rated with another health provider. 9. q The documentation submitted is insufficient. 10. q The health insurer, health benefits plan or health provider has previously been reimbursed. (Proof of date and amount of payment attached.) 11. q Other ________________________________________________________________________ ___________________________________________ A copy of this notice was mailed to the health insurer/health benefit plan on the date indicated. (Proof of service attached.) All further correspondence must be delivered, faxed or mailed to the individual named below: ___________________________________ ________________________________ _______________________________ _______________________ Printed Name Signature Title Date Form Mailed ________________________________________________________________________ __________________________ __________________________ Address (if different from Part I) Telephone Number Fax Number Part III - Request for Arbitration AAA Case No.________________ q No objection has been mailed or payment made within 50 business days after the date of mailing of Request for Reimbursement Form. q The undersigned requests impartial examination of the bill(s) to which the workers compensation carrier objected in Part II above. Arbitration is requested on q All bills/issues q The following bills/issues only: ______________________________________________________________ ________________________________________________________________________ ______________________________________________________ The undersigned requests (check one): q desk arbitration q oral hearing. Enclosed is arbitration fee of $_______ (See reverse for filing fee information.) Designated locale of oral hearing ____________________________________. A copy of this notice and attached documents was mailed to the above-named carrier or (if objection has been timely received) to the individual named in Part II. (Proof of service attached.) _____________________________________________ _____________________________________________ __________________________________ Printed Name Signature Title _____________________________________________ ______________________________________________ __________________________________ Date Form Mailed Telephone Number FAX Number _____________________________________________ ________________________________________________________________________ __________ Name of Representative Address of Representative _________________________________________ _______________________________________ Representatives Telephone Number Representatives FAX NumberPrescribed by Chair, Workers Compensation Board HIMP-1 (10-04) State of New York American LegalNet, Inc. www.USCourtForms.com<<<<<<<<<********>>>>>>>>>>>>> 2 INSTRUCTIONS Requests for reimbursement by a health insurer or health benefits plan ["Plan"] for payments made to health providers on behalf of injured employees entitled to workers compensation benefits, and requests for arbitration of disputed requests for reimbursement, shall be submitted and processed in accordance with the provisions of Subpart 325-6 of Title 12 NYCRR. ALL PARTIES TO WHOM THESE RULES ARE APPLICABLE SHOULD THOROUGHLY FAMILIARIZE THEMSELVES WITH THE RULES, AS THE INSTRUCTIONS HEREIN ARE INTENDED AS A PROCEDURAL GUIDE AND ARE NOT TO BE CONSTRUED AS A COMPREHENSIVE INTERPRETATION OF THE RULES REQUIREMENTS. To All Plans: Requests for reimbursement must be submitted to an employer, workers compensation carrier or special fund ["carrier"] on this form, completed with such information as required on Part I of this form, together with the documentation specified in Section 325-6.3(b). A Plan must send requests for arbitration within 90 calendar days after the earlier of the date on which a carrier has mailed a notice of objection to a request for reimbursement or has failed to make payment or failed to
Related forms
-

New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/