

Last updated: 6/20/2023
Notice To Liable Political Subdivision Or Unaffiliated Ambulance Service {VAW-1}
Start Your Free Trial $ 13.99What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
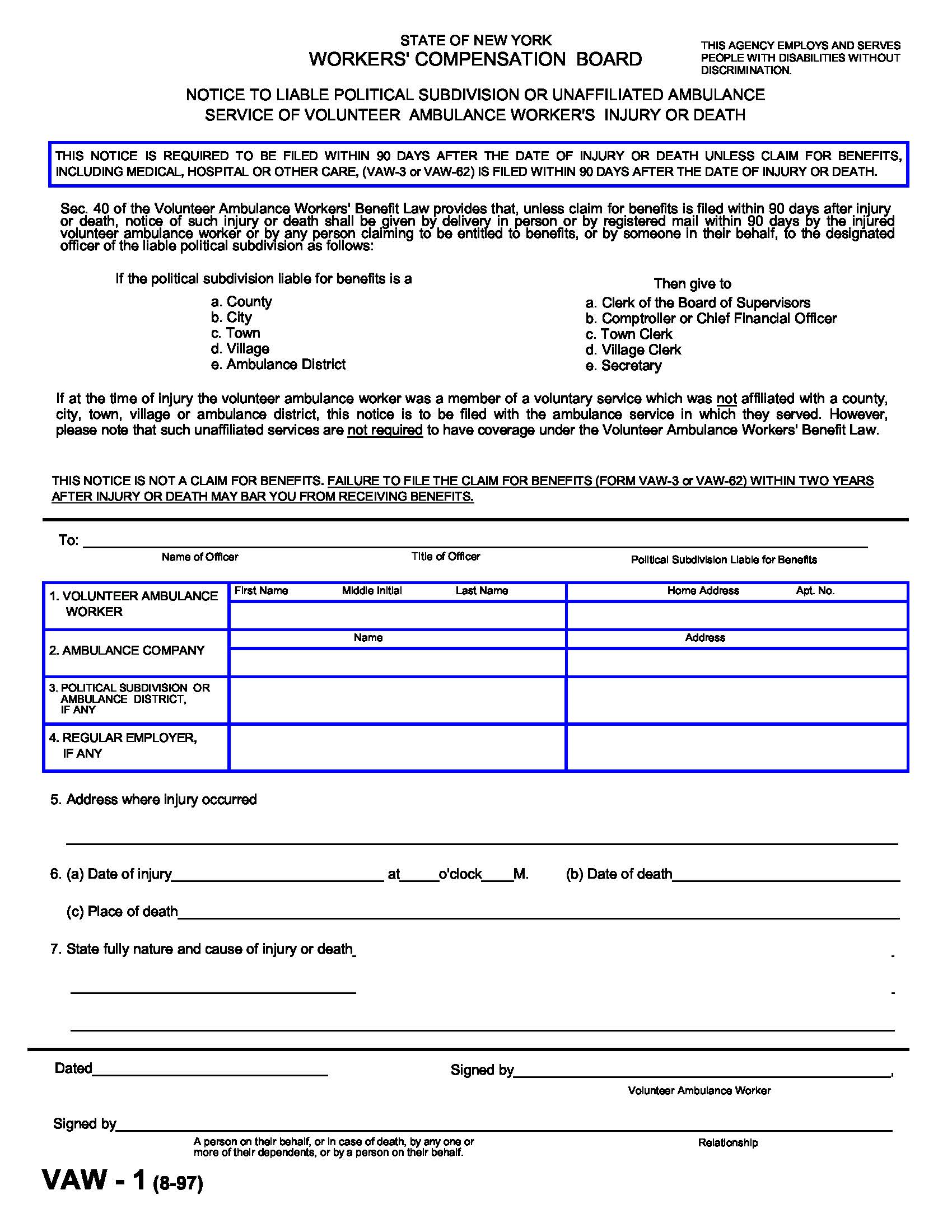
VAW-1 - NOTICE TO LIABLE POLITICAL SUBDIVISION OR UNAFFILIATED AMBULANCE SERVICE OF VOLUNTEER AMBULANCE WORKER'S INJURY OR DEATH. This form is used in the state of New York. The notice must be filed within 90 days after the date of injury or death, unless a claim for benefits has already been filed within that timeframe. The form specifies the designated officer of the political subdivision or ambulance service who should receive the notice based on the type of political subdivision. If the volunteer ambulance worker was a member of an unaffiliated service, the notice should be filed with that ambulance service. It's important to note that unaffiliated services are not required to have coverage under the Volunteer Ambulance Workers' Benefit Law. The form emphasizes that the notice is not a claim for benefits and reminds the recipient to file a claim within two years after the injury or death to avoid potential loss of benefits. The form includes spaces to fill in details such as the names and addresses of the volunteer ambulance worker, the ambulance company, the political subdivision or ambulance district, and the regular employer (if applicable). It also requests information about the date, time, and place of the injury or death, as well as a description of the nature and cause of the injury or death. The form must be signed by the volunteer ambulance worker or a person acting on their behalf, along with indicating their relationship to the worker in case of death. www.FormsWorkflow.com
Related forms
-

New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/7 Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/ -
New York/Workers Compensation/